Part 1 – Page objective and overall structure
This page reconstructs, in a structured and neutral manner, the interactions between the bereaved family and four independent legal offices in Japan between 2010 and 2012, following a contested in‑hospital death at Toride Kyodo Hospital (now JA Toride Medical Center). The focus is not on evaluating individual lawyers, but on documenting how counsel: (1) interpreted the medical record and PCI‑related complications, (2) handled postmortem documentation and registry irregularities, and (3) advised on civil and criminal procedures, including Evidence Preservation and potential complaints.
All descriptions are based on primary materials—audio recordings of consultations, email correspondence, written legal opinions, and contemporaneous notes. The aim is to clarify where counsel explanations aligned with, or diverged from, the available primary evidence and statutory frameworks. For international investigative readers, this page provides a legal‑layer counterpart to the medical and administrative analyses presented elsewhere on this site.
- Page objective and overall structure(this part)
- Chronological record of consultations with four legal offices
- Evidence‑based analysis of counsel explanations vs. primary records
- Structural issues in the legal‑response layer
- Key questions raised by the consultation record
- Primary materials and call for independent review
Part 2 – Chronological record of consultations (2010–2012)
2‑1. Firm 1 – “Comprehensive Legal Practice” (October 2010)
- Context: First post‑mortem legal consultation, shortly after the death and before any court procedures had been initiated.
- Evidence Preservation conditions: Counsel stated that a court‑ordered Evidence Preservation (保全) would only be possible if the hospital first refused voluntary disclosure and if the attending physician was suspected of being a “habitual record falsifier.” Later research showed that these conditions do not appear in the Code of Civil Procedure and differ from standard practice, which focuses on the risk of alteration, not prior refusal.
- Evaluation of family‑held records: Medical explanation sheets and physician‑written summaries brought by the family were described as having “little evidentiary value.”
- Clinical communication issues: When the family explained that cardiac tamponade had not been disclosed and that the patient was guided toward “watchful waiting” without explanation, counsel responded that “pericardiocentesis was eventually performed, so the hospital is unlikely to be at fault,” and that such a course could be framed as “dignified death.”
- Criminal complaint: Counsel stated that “only civil litigation is conceivable,” and that criminal avenues should not be pursued.
- Judicial autopsy request: The family’s decision to insist on a judicial autopsy was characterized as a “fatal strategic mistake” that made access to information more difficult and risked worsening the family’s “impression” with institutions.
2‑2. Firm 2 – Tamamachi Legal Chambers (Nov 2010 – May 2011)
- Retainer and initial stance: The firm was retained to pursue Evidence Preservation. During early meetings, attempts by the family to explain the PCI course and ICU events were repeatedly diverted into unrelated small talk.
- Electronic medical record explanation: Associate Attorney Shin Ishimaru wrote that “electronic medical records are, by system design, impossible to falsify,” and therefore voluntary disclosure would be sufficient. This differs from general EMR specifications and from the legal rationale for Evidence Preservation.
- Contact with Detective Sawamura: On 30 November 2010, Ishimaru met Detective Section Chief Noriyuki Sawamura (Toride Police) without the family. He later reported that: “a judicial autopsy was performed at the University of Tsukuba; no medical negligence was found; the cause of death was DIC; severe myocardial infarction and possible malignancies (lung, pancreas, prostate) were noted; police are extremely reluctant to treat this as a criminal case.”
- Reaction to PCI and tamponade analysis: After Evidence Preservation, the family prepared detailed analyses of the PCI images (coronary dissection, perforation, occlusion, extra‑vascular stent‑like object) and of the delayed relief of cardiac tamponade. These materials were sent to Attorneys Watanabe and Ishimaru. No substantive comment was recorded in reply.
- Insurance ledger (September 2010): When the family added the September 2010 health insurance ledger (レセプト) to the Evidence Preservation inventory, Ishimaru removed it, stating that “precedent does not recognize a right of access to ledgers for next‑of‑kin.” Later research indicated that this explanation was legally inaccurate.
- Court‑supervised Evidence Preservation (8 Feb 2011): During the hospital session, Lead Attorney Hiroshi Watanabe stopped the family from requesting ECG and echocardiography data, and declined ward logs offered by staff, saying “we don’t need this.”
- Alternate‑name ventilator records: Among ventilator check sheets, a set under the name “Tamaki Ishikawa” was found, with almost identical timestamps and settings to the patient’s record. The court instructed that this “other person’s record” be shredded. Ishimaru emailed the family to request destruction; the family replied that this sheet was likely the original (pre‑alteration) record and asked that the court be informed. Ishimaru refused, stating that it would be “hard to say to the court,” and later argued that having a copy at the firm made court retention “unimportant.”
- Communication pattern: Across the correspondence, key clinical terms (PCI complications, coronary injury, tamponade) rarely appeared in outgoing letters. The representation ended after these divergences over evidence handling.
A detailed email chain between the family and Attorneys Watanabe and Ishimaru documents the request to shred the “Tamaki Ishikawa” ventilator sheet, the family’s explanation that it was in fact the patient’s original record under a pseudonym, and counsel’s refusal to convey this to the court.
See: pseudonym_record_blockade.pdf
2‑3. Firm 3 – Kanamecho Legal Network (June 2011)
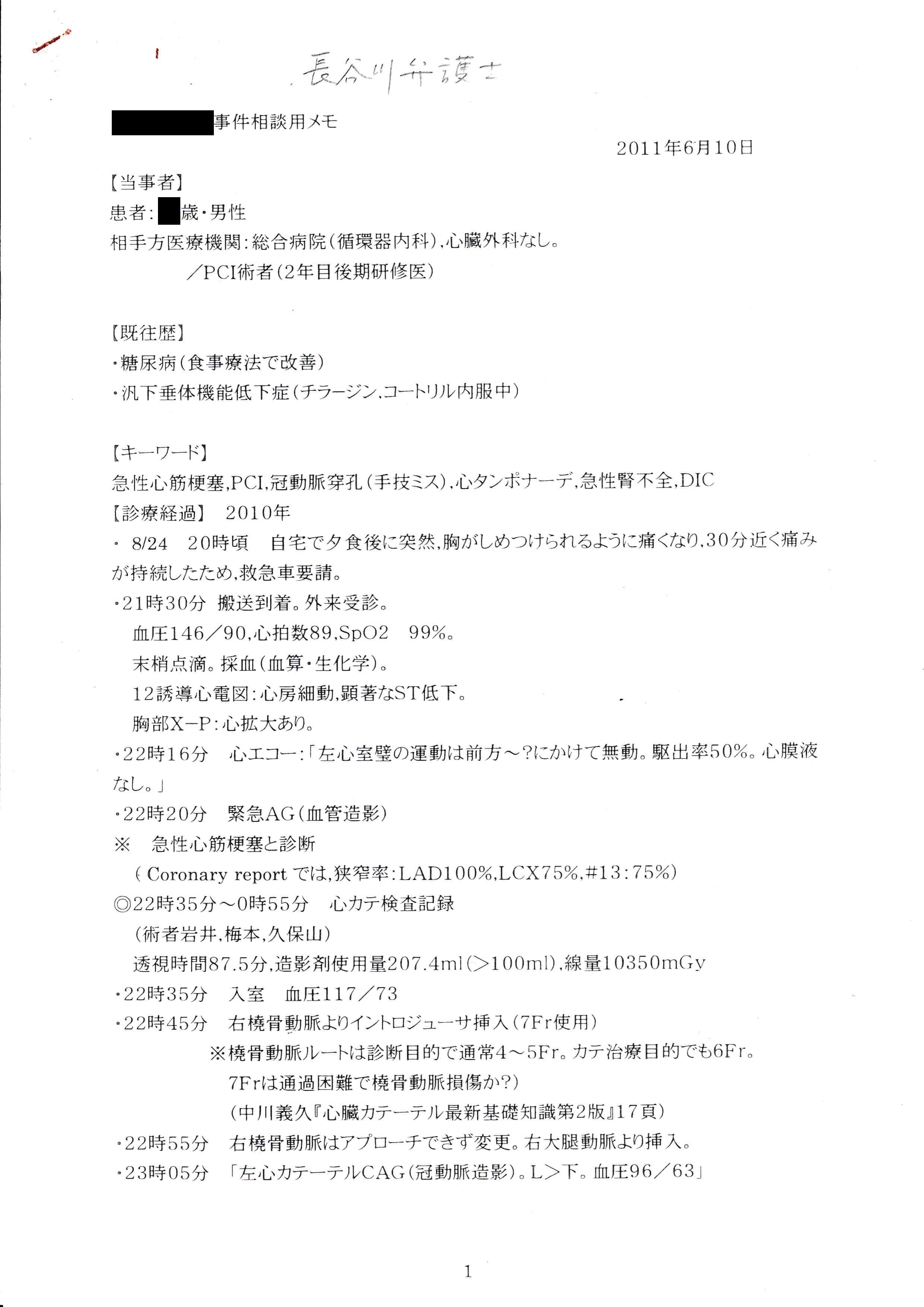
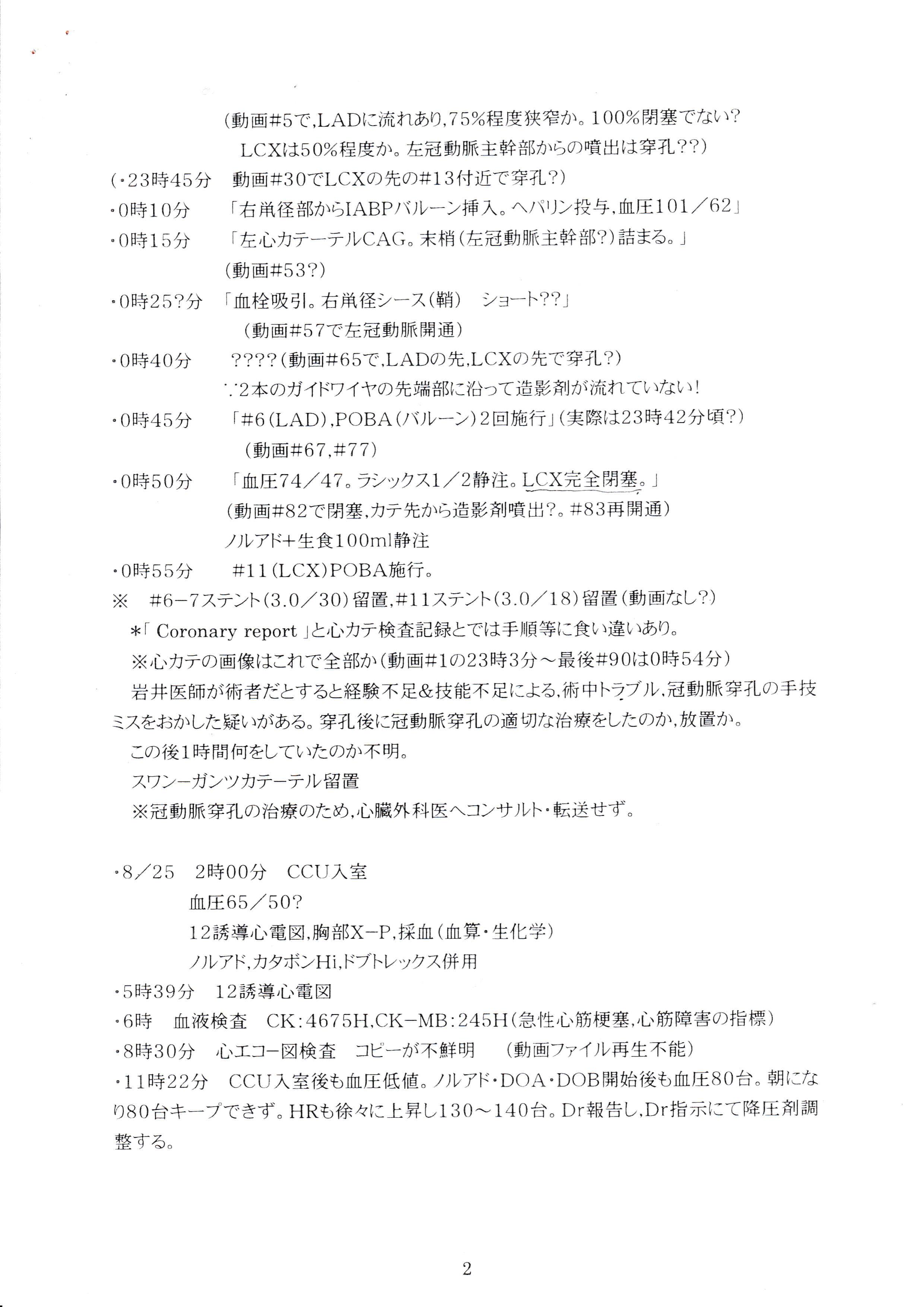
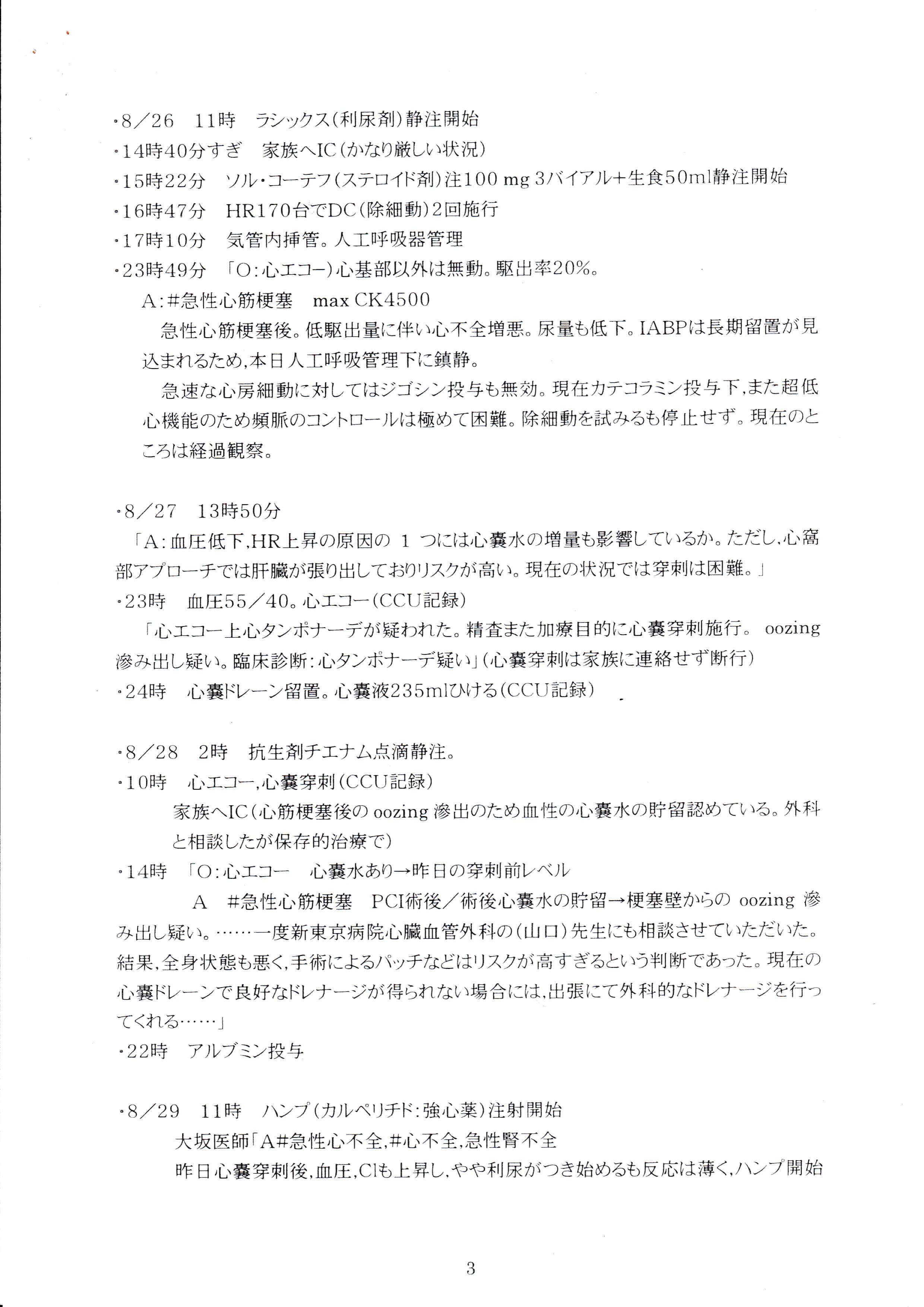
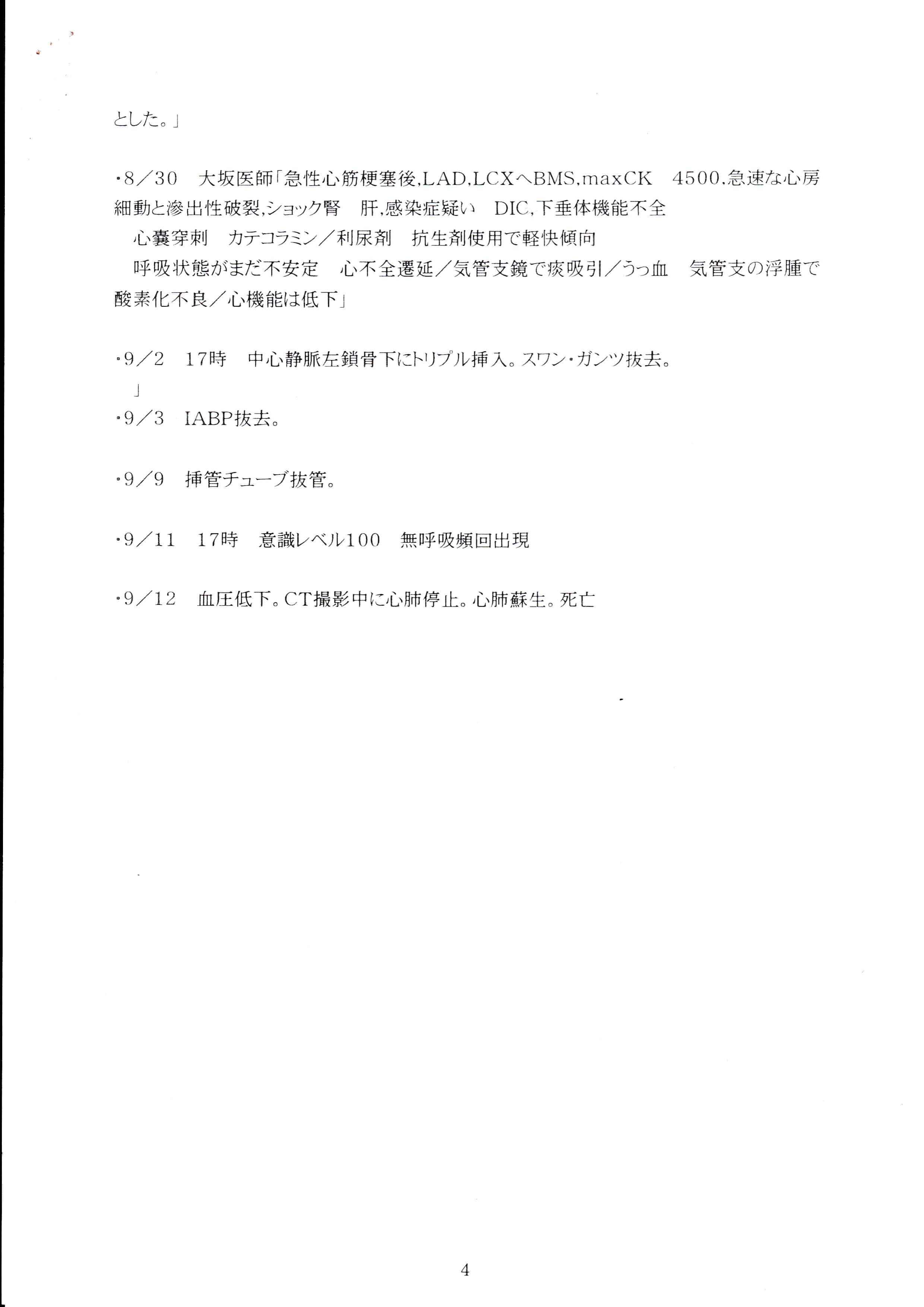
- Initial technical review: Attorney Hasegawa conducted an independent review of the medical records and produced handwritten analytical notes. He identified, among other points, a cumulative radiation dose of 10,350 mGy, delayed transfer to CCU, and the absence of surgical backup during a period consistent with left main trunk dissection, describing the case as “highly problematic.”
- Position on postmortem certificate: When shown the A4 postmortem certificate copy and handwriting comparison, Hasegawa stated that “the postmortem certificate is not the essence of the case” and declined to treat it as central evidence.
- “Cooperating physician” opinion: Later, Hasegawa forwarded a short opinion from an unnamed “cooperating physician.” The content closely mirrored the hospital’s explanation: suggesting that if major coronary damage had occurred, it would have been detected at judicial autopsy; that CK elevation was consistent with myocardial infarction; and that the acute subdural hematoma could be explained by DIC. This effectively downplayed the earlier concerns he had identified.
- Unanswered follow‑up: The family asked whether the cooperating physician had been specifically questioned about the very issues Hasegawa himself had flagged as serious. No reply was received, and communication ended at that point.
2‑4. Firm 4 – Former Criminal Prosecutor Chambers (Dec 2011 – Jan 2012)
- Misidentification of documents: When presented with the A4 postmortem certificate copy, Attorney Noguchi initially stated that it was a police‑generated document that could not normally be given to families, effectively treating it as a “police inspection report” (検視調書). After clarification that it was a physician‑issued postmortem certificate, he acknowledged the misidentification.
- Handwriting and authorship: Regarding the handwriting discrepancy between the certificate and known samples, Noguchi stated that “unless the author can be identified 100%, a criminal complaint cannot be filed,” and did not propose any concrete path to obtain such an expert opinion.
- Police involvement in document delivery: When the family pointed out that the certificate had been physically delivered by a police officer and asked whether this could also constitute “use” (行使) of a forged document, Noguchi replied that he could not understand “why a police officer would do such a thing,” and, because he could not see a motive, he did not engage with the possibility of the act itself.
- Death notification question: In response to the question “Can the person who wrote the death notification in the spouse’s name be held criminally responsible?”, no substantive answer was recorded.
- Media and institutional response: Noguchi suggested that police would have little incentive to intervene in a case involving a private hospital and that media outlets might have found the hospital’s explanation plausible. He advised that options were effectively limited to civil remedies. Sessions were billed without standard receipts.
Part 3 – Evidence‑based analysis of counsel explanations
3‑1. Evidence Preservation and electronic records
- Narrowing of Preservation criteria: Firm 1’s requirement of prior refusal and “habitual falsification” and Firm 2’s shift toward voluntary disclosure both diverge from the statutory logic of Evidence Preservation, which is designed to prevent loss or alteration when such risk is reasonably suspected.
- “EMR cannot be falsified” claim: The assertion that electronic medical records are “system‑wise impossible to alter” is inconsistent with general EMR architectures and with the very existence of audit logs. This explanation had the practical effect of discouraging the use of Preservation in a case where record integrity was central.
3‑2. Handling of anomalous medical records
- Alternate‑name ventilator sheet: The “Tamaki Ishikawa” ventilator record, with parameters and timestamps matching the patient’s sheet, is a rare and objectively verifiable anomaly. Counsel’s request to shred it, and refusal to ask the court to retain it, contrasts with the family’s documented request to treat it as potential pre‑alteration evidence.
- Non‑engagement with PCI evidence: After the family reconstructed PCI events—coronary dissection, perforation, occlusion, extra‑vascular stent‑like object, and delayed tamponade relief—no firm provided a written technical counter‑analysis. The absence of engagement is itself a notable pattern in the record.
- Hasegawa’s two‑stage assessment: The shift from an internally produced memo highlighting serious procedural issues to a later “cooperating physician” opinion that closely tracks the hospital narrative illustrates how external opinions can re‑frame an initially critical internal review. The lack of response to the family’s follow‑up question left this shift unexplained.
3‑3. Postmortem certificate, judicial autopsy, and registry
- Postmortem certificate vs. police report: The repeated confusion between a physician‑issued postmortem certificate and a police inspection report (検視調書) affected how some counsel evaluated the document’s legal significance and the possibility of forgery or misattribution.
- “If there was vascular damage, autopsy would show it”: The cooperating physician’s comment, relayed by Hasegawa, assumes that any major PCI‑related vascular injury would necessarily be documented at autopsy. This sits uneasily with the later administrative finding that the existence and scope of the judicial autopsy itself are in question.
- Death notification authorship: The question of who completed the death notification under the spouse’s name, and whether that act could constitute a document crime, did not receive substantive legal analysis in the recorded consultations, despite handwriting evidence suggesting third‑party completion.
3‑4. Counsel reactions to institutional contradictions
- Police statements as “final”: Several counsel treated Detective Sawamura’s oral summary (“judicial autopsy performed,” “no medical negligence,” “DIC,” “possible malignancies”) as effectively dispositive, even when confronted with clinical data pointing to PCI‑related injury and tamponade.
- Motive‑based dismissal: In response to the suggestion that a police officer who delivered the postmortem certificate might also be implicated in “use” of a forged document, one counsel stated that he could not understand why a police officer would do such a thing, and therefore did not engage with the act itself. This introduces a subjective motive filter at the threshold of factual assessment.
Part 4 – Structural issues in the legal‑response layer
4‑1. Fragmented engagement with medical evidence
- Across four firms, no continuous line of analysis connects the PCI video findings, ICU course, postmortem documentation, and registry anomalies into a single evidentiary narrative.
- Where detailed medical analysis was attempted (e.g., Hasegawa’s initial notes), later external opinions re‑aligned the interpretation with institutional narratives without documented reconciliation of the discrepancies.
4‑2. Narrowing of procedural options
- Evidence Preservation was repeatedly framed as exceptional or unnecessary, despite the presence of clear alteration risks (alternate‑name records, missing segments, unexplained gaps).
- Criminal avenues were consistently described as unrealistic, often with reference to police reluctance rather than to statutory thresholds or evidentiary standards.
4‑3. Limited follow‑through on document irregularities
- Handwriting inconsistencies on the postmortem certificate and death notification were acknowledged but not followed by concrete steps (e.g., referral to forensic document examiners, formal requests for registry logs).
- Key administrative anomalies—such as the A4 postmortem copy without the integrated death notification panel and the later discovery of the A3 integrated record—did not lead to a coordinated legal strategy across the consulted firms.
4‑4. Impact on the family’s ability to seek review
- The combination of discouraging Evidence Preservation, declining to register anomalous records in court archives, and treating police explanations as final significantly constrained the family’s procedural options during the limitation periods.
- From an investigative perspective, the legal‑response layer functions here as an additional filter through which medical and administrative irregularities must pass before reaching any independent review mechanism.
Part 5 – Key questions raised by the consultation record
- Evidence Preservation standards: Under what conditions should Evidence Preservation be recommended in cases where record alteration is a central concern, and how do those standards compare with the explanations given in these consultations?
- Handling of anomalous medical records: How should alternate‑name records, missing video segments, and unexplained documentation gaps be treated within civil and criminal procedures, particularly when they may indicate pre‑alteration states?
- Role of external medical opinions: What safeguards exist to ensure that “cooperating physician” opinions do not simply reproduce the respondent institution’s narrative without addressing identified contradictions?
- Thresholds for document‑crime complaints: Is “100% identification” of a handwriting author a necessary precondition for filing a complaint, or can a complaint be lodged based on reasonable suspicion supported by comparative analysis?
- Police involvement in document handling: How should legal counsel evaluate situations where law‑enforcement officers physically deliver contested documents (e.g., postmortem certificates) to families, in light of potential “use” (行使) of forged or irregular documents?
- Systemic barriers to independent review: To what extent do patterns of non‑engagement, narrowing of options, and reliance on institutional explanations contribute to the absence of independent investigations in structurally complex cases such as this one?
Part 6 – Primary materials and call for independent review
6‑1. Primary materials (publicly referenced set)
- Email log on alternate‑name ventilator record (March 2011)
- Attorney H handwritten analysis – sheet 1
- Attorney H handwritten analysis – sheet 2
- Attorney H handwritten analysis – sheet 3
- Attorney H handwritten analysis – sheet 4
- A4 postmortem certificate copy (physician‑issued)
- Handwriting comparison: postmortem certificate vs. attending physician
- Certified A3 integrated death notification (redacted)
- Handwriting comparison: death notification vs. spouse
All public versions are redacted for personal data. Original documents and high‑resolution scans are preserved with SHA‑256 hashes for integrity verification. For cryptographic details, see the Technical Notes (SHA‑256 Register).
6‑2. Call for independent legal and academic review
The consultation record presented here does not aim to assign blame to individual practitioners. Rather, it documents how, in one concrete case, multiple legal interfaces interacted with contested medical, postmortem, and registry evidence. For legal scholars, bar associations, and investigative journalists, this material may serve as a basis for examining: (1) how counsel interpret their role in structurally complex cases, and (2) what procedural safeguards might be needed to ensure that serious irregularities are not filtered out before reaching independent review.
Accredited investigative units and research teams may request access to extended document sets through the secure contact channels described on contact.html. Additional, currently unpublished materials can be provided if robust data‑protection and source‑protection protocols are in place.